

BY ELI RAMI
ZIKV, more commonly known as the Zika virus, has quickly evolved from a little-researched virus into a global public health threat. Virologists first discovered the pathogen during the late 1940s in a species of monkey that inhabits Uganda’s Zika forest. For decades, scientists believed that ZIKV was a mosquito-borne virus that could only be transmitted to monkeys and mice.1 Even after that theory was disproven, prior to 2007, a total of only fourteen cases of ZIKV in humans had been documented.2 As a result of Zika’s low infection rates in humans, research on the virus remained virtually nonexistent for decades.
Today, with a ZIKV epidemic raging in the Americas, over 1.5 million cases have occurred in Brazil alone. The virus most likely arrived in the Americas during the 2014 World Cup, carried by a visitor from a region such as Africa or the South Pacific, in which the virus is endemic.3 Zika had never before traveled to the Americas, so individuals in the region had not acquired immunity to the disease. Their vulnerability to the virus has allowed it to spread rapidly. For most individuals, ZIKV infection leads to relatively harmless symptoms: a slight fever, a headache, and muscle pain, all of which last for a few days and easily go away with rest. Only one in five individuals infected with the virus become symptomatic. For women, however, the disease has transformed the normally exciting process of pregnancy into a dangerous guessing game—one that can quickly transform into a nightmare. The Zika virus has been determined to cause microcephaly, a disorder in which infants are born with abnormally small heads. Microcephaly reduces life expectancy and causes severe intellectual disability, difficulties with movement and balance, hearing loss, vision problems, and speech problems. The microcephaly epidemic has developed alongside the ZIKV one, with 2,782 cases of microcephaly in 2015 compared to only 147 in 2014.1 The birth defects of children born to Zika-infected mothers have inspired several Latin American governments and public health agencies, most notably those of El Salvador, Colombia and Jamaica, to advise women to delay childbirth for two to three years.
While Zika may have found itself a new home in the Americas, the history of one long-forgotten epidemic, which occurred over fifty years ago in the United States, could inform our way of thinking about the virus terrorizing Latin America today. Rubella, an airborne disease that has been all but eradicated in the Americas, once devastated our country. Between 1964 and 1965 alone, over 12.5 million cases of rubella emerged across the United States. Like Zika, rubella’s primary symptoms are quite mild in the general population. Most symptomatic individuals develop a mild fever, respiratory problems, and a red-colored rash that begins on the face and spreads downward over the body. The most dangerous effect of rubella, however, attacks the very population that is devastated by the Zika virus: pregnant women. These women experience a condition known as Congenital Rubella Syndrome (CRS), in which the rubella rubivirus passes from mother to fetus. When a woman contracts rubella early on in her pregnancy, the likelihood of infecting her fetus rises to 90%.4
In the devastating rubella rampage of the 1960s, one that can now be called “the forgotten epidemic,” over twenty thousand children were born with birth defects such as blindness, deafness, and heart deformities. During the epidemic, the majority of infected newborns displayed signs of mental retardation. Many infants affected with CRS were stillborn or died shortly after birth. During the height of the epidemic, images of children with deformed bodies circulated throughout print and television media. The American public learned to recognize images of spotted infants with “blueberry muffin rash,” dark greyish spots under the skin that appear as a result of CRS. Infected children also held the risk of propagating the virus, often to their own or other mothers. Most infected women acquired the virus from affected children with whom they interacted. Children became both the victims and the threat. While infected children posed significant danger to women during the epidemic, they simply could not be avoided. With women mainly employed as school teachers, retail clerks, and nurses—those professions deemed “suitable” for them at the time—interacting with children often represented a significant aspect of daily life.

During the rubella epidemic, children born with disabilities such as blindness, deafness and mental retardation faced severe social stigma, so women often chose to not bring their babies into the world. Many women infected with rubella were encouraged to abort their children due to the incredibly high risk of birth defects. During the height of the epidemic, over eleven thousand abortions occurred, many of them performed after women were informed of the risks regarding rubella exposure during pregnancy.2 Miscarriages also occurred spontaneously as a result of maternal rubella infection. State governments strongly encouraged parents to place their disabled, CRS infected children in special, state-run institutions. Not only did the disabled children face dire living conditions within these institutions, but they also struggled later in life. Reports of abuse and unsanitary conditions circulated freely within the American public by the end of the decade.
The rubella epidemic of the mid-sixties shaped reproductive laws in the United States. Prior to the epidemic, the public viewed abortion as a crime committed by the Mafia, prostitutes, illegal drug users, and gamblers.5 Furthermore, popular accounts of abortion in magazine and newspaper stories emphasized the risk of women dying. Women who did seek abortions despite legal restrictions discussed their decision only with close family and friends. The rubella epidemic, however, dramatically changed the national discourse on abortion. Physicians faced with the alarming rise of children born with birth defects accepted maternal rubella as a justification for legal therapeutic abortion, as standard medical textbooks at the time endorsed abortion if parents did not want to “…assume the obvious risks…” of having a child born with CRS.6 The epidemic also provoked public mainstream media to discuss the decision to have an abortion, and determine that it belonged to the individual women threatened by the epidemic.
This discourse, however, was not universal. Rubella overwhelmingly affected white, suburban, middle class women. These women presented abortion as a woman’s decision, one to be made in consultation with her doctor and her husband. They received respectful attention from the media, which glorified their motherhood and the plight of their rubella-infected children. At the same time, Black and Latina mothers were demonized—blamed for crime, poverty, and overpopulation during the time of a serious epidemic.6 Women infected with maternal rubella advocated for their right to decide whether or not to abort their rubella-infected fetuses, despite the hoops they had to jump through, mostly instituted by men, before obtaining a safe, legal medical abortion. During the 1960s, many hospitals housed special ethics committees that decided whether or not abortions were medically necessary on a case-by-case basis.6 While therapeutic abortions in the case of maternal rubella passed through the committees with relative ease, not all cases were given equal treatment. Access to therapeutic abortion during the epidemic, almost a decade before the decriminalization of abortion in the Roe vs. Wade decision in 1973, proved exceptionally difficult for the majority of women of color. African American women infected with maternal rubella in the 1960s struggled to access therapeutic abortions. Black women lived in a society that regarded them and their race as negative, criminal and deceitful. While white middle-class suburban women stood at the forefront of the epidemic, medical textbooks at the time did not recognize rubella infection in nonwhite individuals, with one leading pediatric textbook stating, “its identification in Negroes is almost impossible.”6 Women of color were also far less likely to have a doctor who had established relationships with the physicians and hospitals that provided therapeutic abortions—let alone health insurance. As a result, very few nonwhite women were ever deemed “qualified” for a therapeutic abortion; they could not gain the trust of the medical establishment because the medical community questioned their respectability as mothers.7

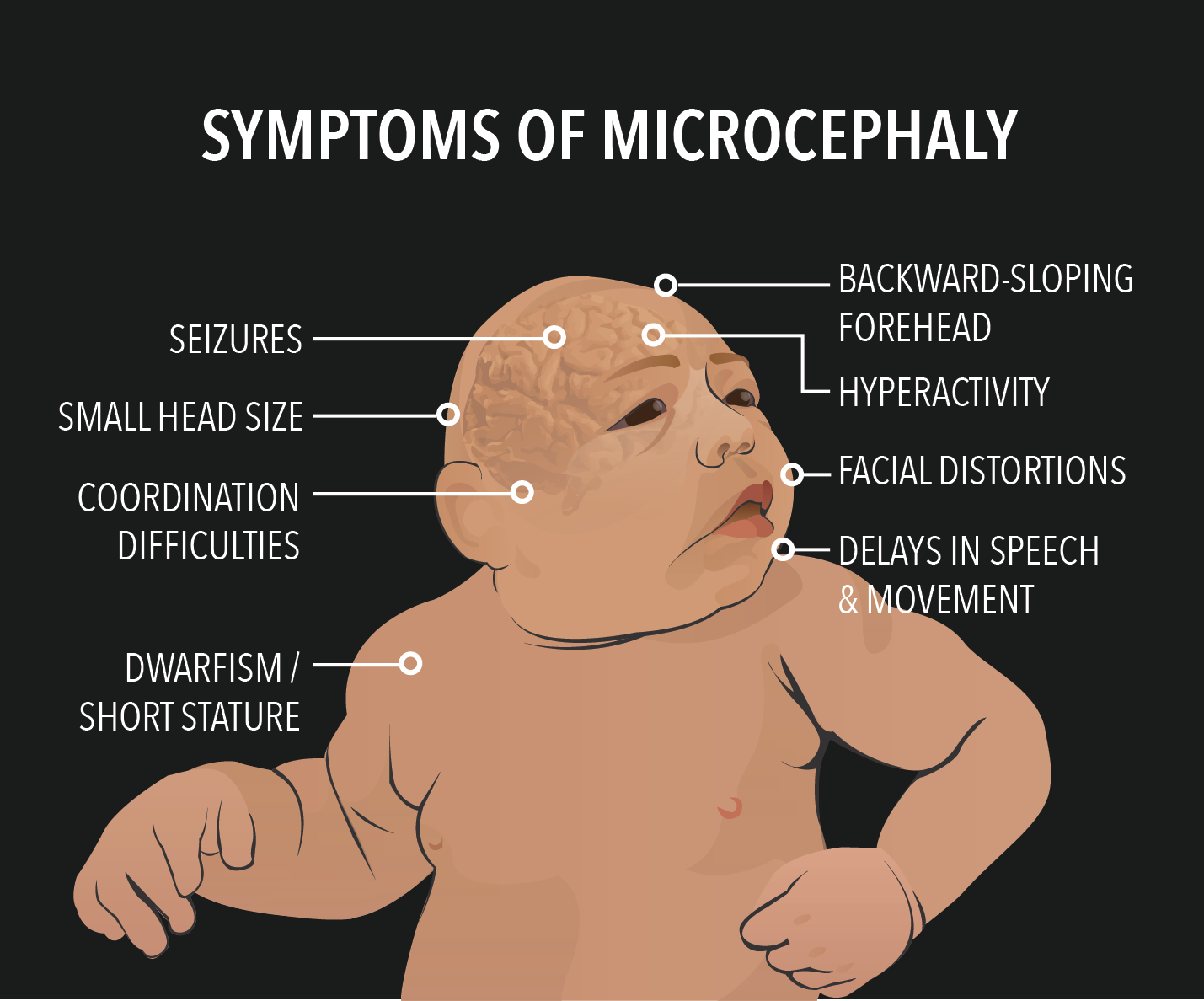
Today, children born with Zika-induced microcephaly face several difficulties. Despite medical advances, many of the complications brought on by microcephaly have no cure or treatment. Before the advent of Zika, microcephaly was an extremely rare condition. As a result, current medical literature on the disorder leaves much to be desired. Children born with microcephaly today face severe intellectual disability, neurological defects and seizure disorders. For example, the face of a child with microcephaly develops a receding forehead because it continues to grow at a normal rate while the head retains its shrunken size. In addition, microcephaly often causes low body weight and dwarfism. Another product of microcephaly, reduced motor skills, can lead to a wide variety of conditions ranging from clumsiness to paralysis.
At the same time, the microcephaly epidemic raises questions of economics and reproduction. The majority of individuals affected by the epidemic live in 24 different countries in Latin America. Countries with the highest rates of suspected infection (Brazil, Honduras, El Salvador and Venezuela) have high rates of poverty among their overall populations. In El Salvador and Honduras, close to forty or sixty percent of the population, respectively, lives below the international poverty line of less than $1.25 per day.8 In El Salvador, where the government has advised women to delay childbirth for two to three years, laws governing abortion are the strictest in the world. Since 1998, the government has restricted abortion in all circumstances, even in cases where pregnancy poses a risk to the life of the mother.9 In many Zika-affected countries, birth control poses a financial burden so significant as to be effectively insurmountable for much of the population. These barriers to healthcare leave many women in Latin America defenseless against the greatest danger of the epidemic: severe birth defects in their children.
In both the rubella epidemic of the 1960s and the ZIKV epidemic of today, children, the most severely affected victims, represent the dangers and unknowns of new diseases. Microcephaly-infected infants, with their clearly visible shrunken heads, have become the face of the current ZIKV epidemic. They grace the news in a manner reminiscent of “blueberry muffin rash.” Both epidemics raise questions of reproductive rights, the social effects of disability, and the long-term treatment of disabled children in larger society. In both epidemics, the burden of disease falls primarily on women and their unborn children. The inequalities of the past strongly echo the issues of the present; many women still lack access to proper reproductive care. Many barriers to necessary health care could be reduced through reforms in public health policy and legislation. While ZIKV may be a new and mysterious disease, we must remember that this situation has manifested within our society before, and ensure that the disabled children of the present are not marginalized like those of the past.
Eli is a freshman in Ezra Stiles college. His major is undecided. He can be contacted at elijah.rami@yale.edu.
____________
References:
- Sikka, V. et al. (2016). The emergence of zika virus as a global security threat: A review and a consensus statement of the INDUSEM Joint working Group (JWG). Journal of Global Infectious Diseases, 8(1), 3-15.
- Rubella: Symptoms and Causative Agent. (n.d.). The History of Vaccines, an educational resource by the College of Physicians of Philadelphia. Retrieved from http://www.historyofvaccines.org/content/articles/rubella.
- Rubella Fact Sheet 367 (2016). World Health Organization. Retrieved from http://www.who.int/mediacentre/factsheets/fs367/en/.
- Reagan, L. J. (1996). When Abortion Was a Crime: Women, Medicine, and Law in the United States, 1867-1973. Berkeley: University of California Press.
- Reagan, L. J. (2010). Dangerous Pregnancies: Mothers, Disabilities, and Abortion in Modern America. Berkeley: University of California Press.
- Northington, V. G. (1997). Under the shadow of Tuskegee: African-Americans and Healthcare. American Journal of Public Health, 87(1).
- World Bank Open Data. (n.d.). Retrieved from data.worldbank.org.
- Abortion Policies: A Global Review. (n.d.). United Nations. Retrieved from http://www.un.org/esa/population/publications/abortion/profiles.htm.
References
- Sikka V, Chattu, Popli RK, Galwanker SC, Kelkar D, Sawicki SG, Stawicki SP,
Papadimos TJ (2016). The emergence of zika virus as a global security threat: A review
and a consensus statement of the INDUSEM Joint working Group (JWG). Journal of
Global Infectious Diseases, 8(1), 3-15.
- Rubella (n.d.). Retrieved from http://www.historyofvaccines.org/content/articles/rubella
- Rubella fact sheet 367 (n.d.). World Health Organization. Retrieved from
http://www.who.int/mediacentre/factsheets/fs367/en/
- Reagan, L. J. (1996). When Abortion Was a Crime: Women, Medicine, and Law in the
United States, 1867-1973. Berkeley: University of California Press.
- Reagan, L. J. (2010). Dangerous Pregnancies: Mothers, Disabilities, and Abortion in
Modern America. Berkeley: University of California Press.
- Northington, V. G. (1997). Under the shadow of Tuskegee: African-americans and
health care. American Journal of Public Health 87(1). 1774.
- World Bank Open Data (n.d.). Retrieved from data.worldbank.org
- Abortion Policies: A Global Review. (n.d.). United Nations. Retrieved from
http://www.un.org/esa/population/publications/abortion/profiles.htm
