
BY CANDICE HWANG.
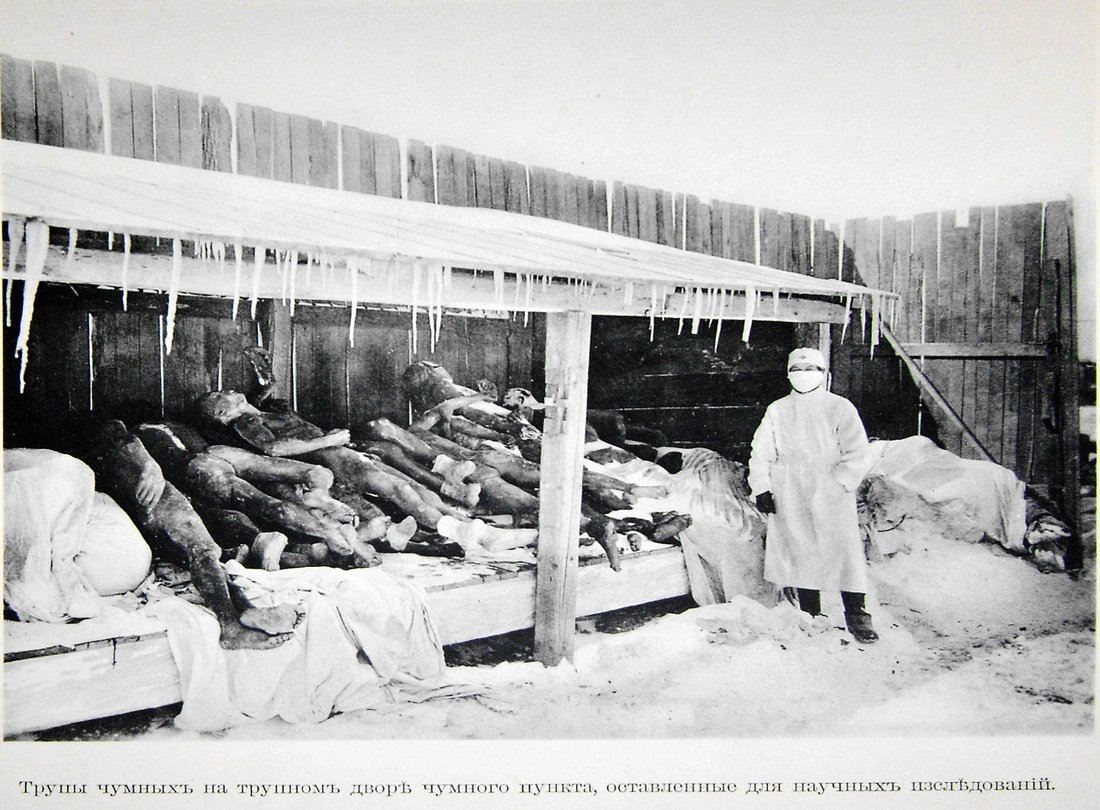
Photography courtesy of Harvard University Library.
** This essay by Candice Hwang won the third place prize in the Yale Global Health Review 2014 Class Essay Contest**
In the 18th and 19th century, there was an influx of Westerners in China, bringing with them their concepts of how state medicine and public health should be run. In Hong Kong, which became a British colony in 1842, the imported British ideas clashed with local traditions and caused conflict over the public health response to the 1894 bubonic plague epidemic (Chan 12). The conflict manifested in placard campaigns mounted by the Chinese against the intrusive measures imposed by the colonialist government of Hong Kong (Benedict 145). On June 11, 1894, this conflict escalated into a Chinese-led mob attack on two American missionary women who were treating plague victims (Benedict 146). The causes underlying this conflict stem from disease framing, power politics, and colonial exceptionalism.
In the late 1800s, two primary forces managed public health in Hong Kong: the first was the British colonial government and the second was the native Chinese “extra-bureaucratic activist elite” (Benedict 131). Starting in the late Ming and early Qing Dynasties, Chinese elites had promoted the shantang, or “benevolent societies”, movement that formed charities and non-governmental organizations all over the country (Smith 309). In Hong Kong, the preeminent shantang responding to the plague was the Donghua Hospital Directorate. The Donghua Hospital dealt with the epidemic by setting up a hospital branch dedicated to treating plague victims with classical Chinese therapies. They also sought to return the sick and dying to their families in Mainland China (Benedict 137). These practices were opposed by the British government, which advocated quarantine and prevented anyone from emigrating. Furthermore, in an attempt to clean up the unsanitary conditions to which the plague was attributed, the British destroyed the entire Taipingshan district of Hong Kong, tearing down three hundred fifty houses and displacing seven thousand Chinese (Benedict 146). As one could imagine, these policies did not foster a peaceable relationship between the locals and the government.
Underlying this conflict between the Donghua Directorate and the British government was the fundamental difference between traditional Chinese medicine and Western biomedicine. The bubonic plague as a disease did not exist in the Chinese medical lexicon. Rather, symptoms of the plague, such as fevers, were seen to be a set of exogenous heat illnesses. In fact, the idea of “disease” is not useful in explaining traditional Chinese medicine, since “unlike biomedicine, which rests on the assumption that motion and change are abnormal and need to be explained, Chinese medicine begins with the proposition that transformation is intrinsic to existence” (Benedict 101). In other words, for the Chinese, a fixed cause-and-effect relationship did not exist for illnesses, and illnesses were not contagious. This way of thinking made it difficult for the Chinese to understand British justifications for quarantine.
The fact that Western biomedicine had not yet found the true physiological cause for the bubonic plague did not help the government’s case. Not until 1898, when Paul Simond published a paper showing how the plague traveled by rat flea, was the microbial cause of the bubonic plague determined. At the time, European sanitarians in Hong Kong still believed miasmas or “bad air” caused the plague (Benedict 141). Westerners regarded their miasma theory as superior because it supposedly relied on empirical proof, unlike Chinese traditional medicine (Macpherson 56). However, it is important to note that this “empirical proof” was based on correlation rather than causation. Indeed, statistics showed how over 2,500 people died of the plague in the unsanitary Chinese neighborhoods, while the total number of cases among non-Chinese was below ten (Benedict 142). But unsanitary environments are not the direct cause of the bubonic plague. At heart, both the Chinese tradition theory of medicine and the Western theory of miasma are human interpretations of worldly phenomena. In fact, the metaphorical similarities are astounding. Europeans conducted massive climatology studies throughout the 1800s to determine the effect of temperature and moisture on various medical conditions (Macpherson 27). In the same vein, traditional Chinese medicine examined the balance of “warm” and “cool” elements of the body. Western biomedicine studied the climate of the land, while traditional Chinese medicine studied the climate of the body. The fact is that the 1894 plague in Hong Kong brought into conflict two systems of disease framing, both of which were ironically unscientific and ineffective against the bubonic plague (Benedict 147). Instead, the weaknesses in each theory left room for each to undermine the other.
Yet the British government insisted on carrying out their policies as a way of asserting political power. The shantang were successful in setting up medical facilities and providing proper methods for removing the dead. However the foreigners living in Hong Kong saw the response as inadequate because it was directed by Chinese civic leaders rather than by British government officials (Benedict 135). Beginning in the 1870s, European sanitarians living in Hong Kong consistently lobbied for the British colonial administration to overhaul the public health system. In response, a permanent Sanitary Board was created in 1883. The power of the Sanitary Board, however, was continuously curbed by local landlords who did not want to expend money to clean up their properties (Benedict 139). The government saw the 1894 epidemic as an opportunity to consolidate power for the Sanitary Board and justify large-scale public health interventions. These included authorized house-to-house searches to remove plague victims or corpses, forced quarantine of suspected plague victims to a factory-turned-hospital, and the aforementioned destruction of Taipingshan district (Benedict 144). All of these actions caused the Chinese to view British authorities as inhumane and hostile to Chinese values.
The colonialist authorities saw no issues with carrying out these changes because they perceived the Chinese as unsanitary and backwards. They perceived themselves to be responsible and knowledgeable as they carried out the “white man’s burden” (Kipling). On a visit to Shanghai, French doctor Paul-Edouard Galle recorded that Chinese housing was extremely overcrowded, with “low, narrow structures packed with numerous families, each occupying just a few square meters” (Macpherson 38). Ventilation was poor, and a foul smell permeated the whole city. Galle also remarked on the filthy living habits of Chinese who “went unwashed from cradle to grave” (Macpherson 38). In line with colonial exceptionalism, the mindset of incoming Europeans was to identify all the deficiencies in foreign cities and mold them to become more like the great cities of Europe.
The British public health interventions in Hong Kong were heavy-handed, insensitive, and informed by faulty science. In the end, however, the public health overhaul did confer benefits to the Chinese in Hong Kong and in other cities around China. By the late 1890s, public health legislation was firmly in place in Shanghai and Hong Kong. Streets were cleaned up and waterworks were installed (Macpherson 267). Even the local Chinese marveled at the changes that Westerners had brought to their cities. As Cheng Kuan-ying and other reformist writers described, “When strangers first come to Shanghai…and see how clean and broad the streets are…they cannot help asking in delight: ‘Who has had the power to do this?’ The answer was the Westerners.” (Macpherson 261) When the next bubonic plague epidemic hit in Manchuria in 1910, the Chinese government put into place Western-style public health institutions to quarantine the disease (Benedict 163). The conflict of 1894 – and its underlying scientific, political, and racial causes – was put aside in face of a new century.
