
BY SARA LOCKE

Khushi Baby is a wearable mHealth platform tracking maternal and child health to the last mile. Its mission is to reduce infant and maternal mortality due to vaccine-preventable disease. As explained in the Khushi Baby 2016 Annual Report, the Khushi Baby system comprises of a culturally tailored NFC necklace, which digitally stores immunization and health records for pregnant mothers and children. The necklace interfaces with a mobile app to update records, and serves as a social symbol of health that can be used to recruit more mothers to immunization camps and antenatal check-ups. The data is synced to a dashboard for health officials to manage care delivery resources. Also, the necklace serves as a social symbol of health that can be used to recruit more mothers to immunization camps and antenatal check-ups. The dashboard sends dialect-specific voice reminders to the family’s cell phone in the local dialect to encourage MCH awareness.
The Khushi Baby concept originated in the Yale University class, “Appropriate Technology in the Developing World.” This class focuses on different global-scale problems. Students were assigned the task of developing vaccine-related innovations that could help prevent the 1.5 million deaths that result each year from vaccine-preventable diseases. While other teams focused on vaccine storage and delivery, Khushi Baby addressed the huge organizational difficulties faced by clinicians and parents as they document a child’s vaccination record. In many rural areas where public immunization rates are extremely low, methods for tracking vaccination history rely on outdated paper forms. Health workers are burdened by this inefficient system. Khushi Baby aims to streamline the data collection process.
In the summer of 2016, I joined Khushi Baby as a Field Research Intern at their Headquarters, in Udaipur, Rajasthan. I am grateful to the Global Health Scholars program for enabling this work. While in Udaipur, I had the opportunity to gain hands on experience with designing and implementing a research study. With the help of Farhana Jamal and Pawan Singh, two members of the Khushi Baby team, we conducted a qualitative study focusing on rural community health workers’ experiences. I conducted the data analysis upon returning to Yale in HLTH 490: Global Health Research Colloquium with the guidance of Professor Elizabeth H. Bradley, PhD. What follows is an abbreviated version of the research paper produced in this class.
The objective of the Indian Government’s National Rural Health Mission (NRHM) is to strengthen the healthcare delivery system in rural India, with a focus on the needs of vulnerable, village populations. In 2005, the NRHM established a new cadre of community health workers called Accredited Social Health Activists (ASHAs) (Bajpai, 2011). ASHAs act as village-level, grassroots workers who link the community to the public health care system by addressing both supply and demand-side issues. ASHAs have three roles: (1) to create awareness on health and its determinants; (2) to mobilize the community towards local health planning; and (3) to increase utilization of the existing health services (Fathima et al., 2015). ASHAs represent the cornerstone of NRHM’s strategy to address the millennium development goals on health related indicators in India (MoHFW, 2005).

Since its implementation in 2005, the ASHA program has been evaluated in numerous studies. The 2011 assessment from the National Health Systems Resource Centre emphasized that while the ASHA program is now operating at scale and serves an integral role in the public health system, the ASHA’s functionality and effectiveness can still be improved (Vedm et al., 2011). A further study found that the ASHA program increased immunization rates from 12-17%, but only in Indian states that give a focus to the program (Gopalan et al., 2012). Additional studies examined incentives, recruitment, roles and responsibilities, supervision, and training for ASHAs throughout India. The research emphasizes a need for stronger ASHA supervision and support, with clearly defined roles and responsibilities for all frontline health workers (Bajpai, 2011; Fathima, 2015; Singh, 2010; Rahman, 2010). Despite the usefulness of these findings, only one study of those reviewed report on the ASHA’s own views of their roles (Scott & Shanker, 2010). This specific study involved 25 interviews and 5 focus groups with ASHAs, health professionals and community members as well as over 100 hours of non-participant observation at public health centers. The research investigated contextual features of the ASHA program that are hindering the ASHAs’ capacity to improve health outcomes and act as cultural mediators and agents of social change. The study found the ASHAs’ payment remuneration system was inadequate, and that the hierarchical structure within the public health system “limited opportunities for meaningful communication across levels of status, seniority and income” (Scott & Shanker, 2010). The study concluded that progressive policy on community health worker programs must be backed up by more concrete institutional support designed to enable ASHAs to fulfill their roles. Therefore, despite numerous studies of the ASHA program, first-person accounts of the ASHAs’ experiences, including their views on the challenges they face in performing their various roles, remain largely unexplored. In particular, there is a lack of knowledge regarding the ASHA-patient relationship.
With this in mind, the objective of the study is to understand how the ASHAs experience their work, including their perspectives on the challenges they must overcome to execute their duties. A specific focus of the study was to investigate the challenges the ASHAs face in the provision of immunizations and antenatal care for women and children. In the study, qualitative methods were used to capture the voice of the ASHA and to gain a holistic understanding of their role as the primary liaison between rural healthcare providers and the communities they serve. Given the central role ASHAs are intended to play in India’s health system, a deeper understanding of their experiences can help Indian policymakers gain a more comprehensive and valid view of the healthcare delivery system.
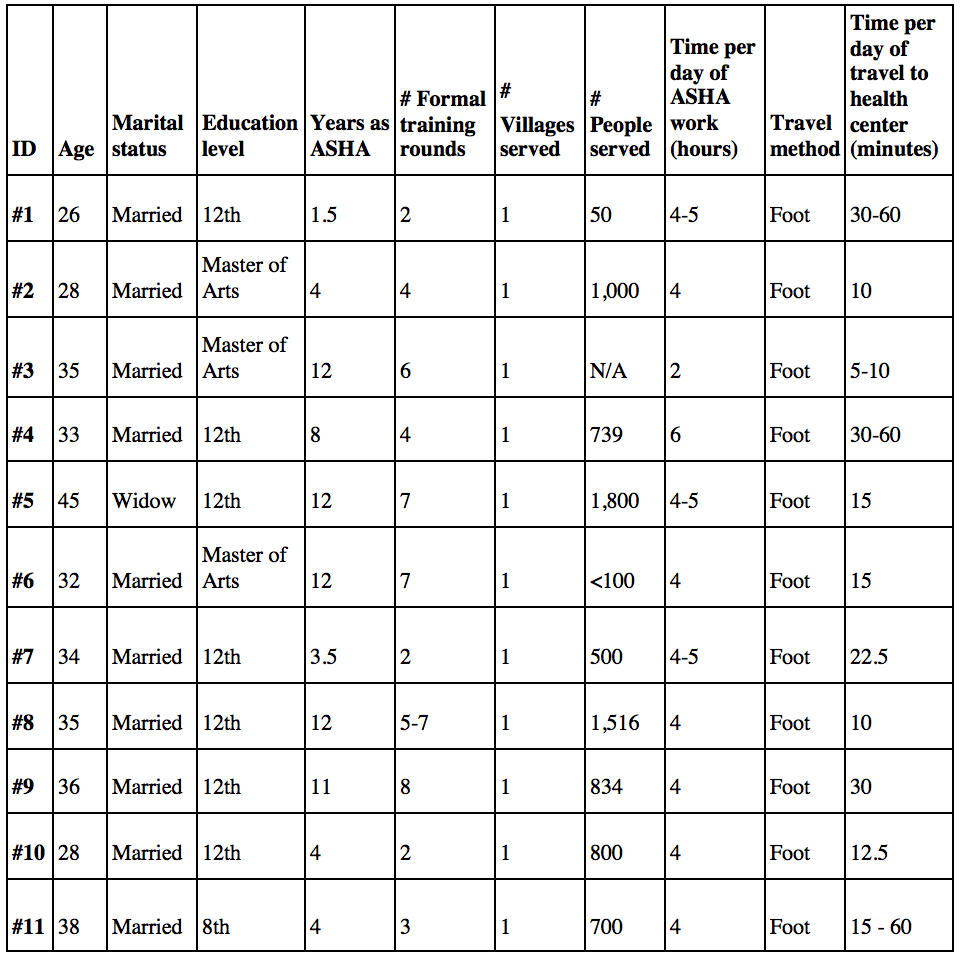
To understand the ASHA’s experience, we conducted a qualitative study with a group of ASHAs working in Udaipur, a city in the western Indian state of Rajasthan. Udaipur is relatively under-researched compared with other regions in India. Qualitative methods are particularly useful for providing in-depth, nuanced understandings of individuals’ experiences and perspectives within local contexts (Ritchie, 2003). Using purposeful sampling to recruit ASHAs, researchers held interviews in situ in the rural villages throughout the region surrounding Udaipur to ensure the sample was reflective of diverse parts of the state.
The final sample size was determined by theoretical saturation regarding questions about the ASHA role and challenges they faced in executing this role. Theoretical saturation was reached when participants were giving very similar answers to the questions. Data saturation was achieved upon completion of 11 participant interviews
Data analysis was performed using factor analysis and constant comparative analysis. The data analysis generated a set of four key concepts, which represent the common view of the interviewed ASHAs that relate to the enablers that facilitate an ASHA’s ability to fulfill her role as a health care provider. The respective barriers to these enablers were also explored. We selected verbatim quotations to illustrate the recurrent concepts. The findings, reported below, are presented using the four factors as sub-headings.
Concept 1: House to house visits
All of the ASHAs described home visits as central to their work and important for their impact on clients and families, particularly for ensuring mothers attended vaccination camps or received antenatal care. ASHAs house-to-house visits are effective for a variety of reasons: crucially, the ability to develop a personal relationship of trust with their patients, and the ability to involve the family.
ASHAs claimed that house-house visits form a relationship of trust between an ASHA and her patients. One ASHA explained that the patients’ trust in her is what motivated them to attend vaccination camps. This trust stemmed from regular, face to face contact:
As we know them and do regular field visits, so they trust us and come here. (ASHA 8)
Two other ASHAs explained that this regular visitation meant they could reinforce the importance of attending vaccination camps or receiving antenatal care.
Those who do not understand, we visit them repeatedly and explain them again and again. (ASHA 11)
Best way is to do home visit again and again. If we will sit with them and will explain and motivate them, then they will understand that if we are coming to them again and again, then there must be something good for the health of their child, that’s why we are coming here. (ASHA 1)
Another participant described these visits as useful because they allowed the ASHA access to her patient’s family. The mother does not make health care decisions alone. Instead, the ASHA emphasized how health care is family decision. For example, one ASHA explained that to convince a mother to attend a vaccination camp, she also had to convince the patient’s family:
Yes, door to door visit and explaining the parents. Visiting them at home is the best way. We have to talk to the family members also because if she is ready and the family members object that where she is going and like that, then she won’t come. So we have to explain them also. (ASHA 7)
Despite the importance of home visits, practical challenges were described as limiting ASHAs’ ability to conduct these visits. A barrier to an ASHA’s ability to conduct her house-house visits was limited time. When we asked one ASHA if there is anything else she would like to discuss, she explained her frustration at having to sit at the vaccination camp (the Aanganwadi centre) when she could be making house-to-house visits. In this case, the ASHA felt she was wasting her time, because her work was in “the field,” in the homes of her patients:
As we sit most of the time at Aanganwadi centre, so we get less time to do household works. We have to manage our children also. Sometime we have to sit unnecessarily at the centre, because we do not have work daily. If we will spend more time in field, then we can be more in contact with the women. If you could help us, then we want that we should not have bonding to sit at the centre even if there is no work here. Our reimbursement is also so low. We are just given Rs. 1600/- and asked to sit at the Aanganwadi for the whole time. So, when will we go to the field and when we will do home visit and gather information. (ASHA 4)
Lack of adequate transportation presented challenges for implementing home visits by the ASHA, and visits to the vaccination camps by mothers. Although forms of transport are available, this does not mean the transport is available when actually needed. One ASHA narrated a story of a patient who was unable to give birth at a hospital, because the ambulance was too slow. In this case, the ASHA was unable to fulfill her role, due to the inadequate infrastructure:
We had 3 home deliveries here at our place after April. In the latest case, when I called 108 ambulance, I got the reply that it’s not working. Then the patient herself called the ambulance, they said that it’s coming from some other place, but by the time it arrived, delivery happened. (ASHA 9)
Closely related to this, another ASHA explained how rough, rocky rural terrain is a serious physical barrier. As aforementioned, all ASHAs included in this study travelled by foot. Yet the homes they are required to visit are often far away, in remote locations. The ASHAs struggle to reach their patients, and likewise, the patients are unable to trek to the vaccination center:
Another problem is distance. As houses are located on hills in the village, so it takes time to reach at the center. Some women got busy in work, so they can’t come. (ASHA 5)
Concept 2: Education
Numerous ASHAs perceived that they play an important role as teachers. ASHAs educate patients about disease. They clarify why vaccinations, and healthcare in general, are important. Moreover, they explain why vaccinations might result in fever, and reassure mothers that this reaction is normal, and not to be feared. By doing so, ASHAs motivate their patients to receive the necessary vaccinations or antenatal care:
Yes, they ask us that our children gets fever after vaccination, then we tell them that when immunization is done for the first time, the child gets fever, but it is for the protection from diseases. We tell them about the diseases. (ASHA 10)
When asked to discuss the difficulties they face in motivating patients to attend vaccination camps or antenatal care, the ASHAs acknowledged that their patients are initially fearful of vaccinations. ASHAs explained that their patients do not understand the fever that often follows an injection, and therefore do not want vaccinations. There is a stigma surrounding vaccinations, which deters patients from seeking care from the ASHA. This fear was often cited as “illiteracy” by the ASHAs. While “literate” women know that vaccinations are effective, “illiterate” women require the assistance of the ASHA:
There are many women who get the vaccination done, but still some women don’t take vaccination, as they are afraid of fever and other things. So we motivate them that this fever is good for you, as it’s bringing out the illness (ASHA 6)
If the mother would be literate, she will bring the child on her own. She will contact us herself, that I want my child to be vaccinated, what should I do. And those who are illiterate, we have to go and explain them and inform them about the vaccines. Literate women are already intelligent. They know that if it’s not done here, then they have to go to Udaipur. For illiterate women, we face problem. We have to tell them because they do not know. (ASHA 1)
If they do not come, we have to visit them again and again. Those who are intelligent, they come and those who are not intelligent, we have to go and call them again and again. Those who understands, they come on their own. But tribal and village people do not understand… because they are not literate. We have to visit them again and again. (ASHA 5)
Moreover, when patients fear the vaccines, they are likely fearful of healthcare providers and healthcare more generally. An ASHA explained how her patients who dislike vaccinations are similarly anxious about hospitals. By consequence, the women are reluctant to give birth in the hospital, preferring to remain at home, in perceived safety:
Some women are afraid of vaccination. Those who regularly take vaccines, they go to the hospital for delivery. But those who don’t take the vaccines, they avoid going to the hospital. She remains afraid. (ASHA 11)
Concept 3: Mothers’ availability
ASHAs stated that their ability to provide health care largely depended on patients’ availability. Numerous ASHAs specified that mothers are often unavailable due to work, or because they are too busy caring for other children. Mothers do not feel they have the time to attend a vaccination camp or receive antenatal care, especially given that they must go more than once. Moreover, mothers are not available when an ASHA makes her house calls. As a result, the ASHA faces difficulty in accessing her patients, and spending crucial face-to-face time with them:
If they have some work at home or if their family member refuses and complains about problems like wasting of time and asks why they go repetitively etc., then the lady doesn’t come. For instance, today I called a lady over phone and then I visited her home also to inform, but she has not arrived yet. Her husband is saying that she will not come, she is getting treatment from some other hospital, so we don’t have time to come here and to go there. And he said that we have some guests also at our home, so she will not come. (ASHA 7)
Village women give more attention on their work and not on their body. They remain engaged in farming works or take care of the children and could not care about themselves. (ASHA 3)
Concept 4: Inconsistent access to medical record information
ASHAs reported that they require adequate medical records about their patients in order to fulfill their roles as health care providers. The NRHM established the use of immunization (MAMTA) cards to record the immunization status of patients in rural areas, carried by the patients themselves. ASHAs explained that they need this documentation to give correct vaccinations. However, some mothers forget to bring their cards, or do not have one. In such instances, while some ASHAs keep personal records of their patients, others will not give treatment to the patient. Therefore, an enabler for ASHAs is to have adequate health records for their patients. They face a decision of whether or not they can give a vaccination without such records.
One ASHA explained that she will give treatment to patients she recognizes, regardless of whether or not the patient brings the MAMTA card. This ASHA keeps her own records about her patients, which she refers to. ASHAs are knowledgeable about the health status of their patients, reinforcing the importance of the house-to-house visits. This ASHA also will refuse to treat patients she does not recognize. Such a decision could have long-term impact for the patients seeking care:
If she forgets [the MAMTA card] than either we tell her to bring the card or as we also do entry in our registers, so we check it in our record and get her vaccinated accordingly.
But if she is an outsider, we return her because we don’t have their records and we don’t know which vaccine is to be given and which is not to be given. If she is from our area, then we know which vaccine is to be given and which not. (ASHA 6)
One ASHA did not keep a personal record of her patients, and depended on MAMTA cards. When a patient did not have her card, even if the ASHA recognized the person, the ASHA refused to give any vaccination at all. This decision was rooted in the desire to deliver appropriate medical service. Yet, without an effective record-keeping system in place, patients are the ones who ultimately face the consequences:
She will not be vaccinated, because it gives the record of all the check-up’s and vaccinations done. A seal is also put for HIV positive or negative on the card. If the woman is HIV positive, then her treatment can be started soon accordingly, so that the child doesn’t get HIV…We refuse. (ASHA 4)
Another ASHA reported that she was able to give a vaccination based upon the child’s age and record the entry later. The purpose of a medical record is to hold up to date, correct information. However, if an ASHA is “doing entry later,” in retrospect, there are some concerns about the accuracy of the information recorded:
Even if they forget to bring the card, we vaccinate them as they have come from far places. Entry can be done later, but it’s important that they came to the camp.
We know because we vaccinate them every month. On the basis of child’s age, we get to know. (ASHA 1)
Discussion
We found the ASHAs play a critical role as a link between the community and the public health care system. Understanding the factors that shape these workers’ experiences is essential for the improvement of the health care delivery. Previous research has focused on the need for strong institutional support for the ASHA program as a whole, prioritizing the need for a better payment scheme, and improving communication between ASHAs and higher tiers of the health care delivery system. Results from our qualitative study provide insights about the ASHAs’ own perspective on the challenges they must overcome to execute their duties as health care providers. Therefore, the presented research explores from a different perspective and in detail why institutional support is necessary for the ASHA program. The study offers a novel understanding of the experiences of the ASHAs, with particular consideration on the ASHA-patient relationship, and how this relationship might be strengthened.
A predominant idea weaving through the four concepts discussed is the importance patients trusting the ASHA. ASHAs endorse house-to-house visits as a central component of their work because this was the “best way” to establish a bond with their patients and an understanding of their patients’ family situation. Additionally, ASHA’s required the trust of their patients to overcome the stigma surrounding healthcare practices, particularly in the issues patients have with antenatal care and vaccination.
The main barrier to creating a relationship of trust was the inability to have face-to-face contact. This was a consequence of the ASHAs’ inability to visit the homes of her patients, either because she was required to sit at the vaccination camp for a certain number of hours or because transport was difficult. It was also a consequence of the patients themselves being unavailable, due to work or other family commitments.
Facilitating ASHA’s ability to create a relationship of trust can markedly influence their impact. An ASHA’s household visit is a mechanism that results in a strong relationship between the ASHA and her patients. Given the importance of these visits, investigating the relative value of the required hours ASHAs must spend at vaccination camps should be a topic of future research. It is possible that with less time required at the camps, ASHAs might gain better access to patients in their homes. Additionally, with better access to patients’ homes, ASHAs might be more likely to enlist the assistance of patients’ families in healthcare decisions. This could strengthen the relationship with their patient, and lead to better health outcomes.
Given that transportation was also cited as a barrier to household visits, this study has illuminated the need for either improved methods of transportation, or more health centers at accessible locations. From the perspective of the ASHA, inadequate transport limited their ability to fulfill their roles. Policy makers should prioritize infrastructure spending tailored toward ambulance availability in rural areas.
ASHAs felt their role as teachers constituted an important factor in fostering trusting relationships with their patients. ASHAs acknowledged the “illiteracy” of their patients as an obstacle. Future research should analyze the most effective methods of education in these communities. Educational materials must be readily available for an ASHA to continue to de-stigmatize health care practices.
It was found that ASHAs lack a uniform medical reporting procedure. Respondents reported that MAMTA cards are not always used. This hinders an ASHA’s ability to deliver appropriate health care services to her patients. A reliable system would ensure all patients who attend vaccination camps are accounted for and receive the appropriate medication. Future research should examine more effective methods of record keeping in rural areas.
Limitations
These findings should be understood in light of three main limitations. First, the sample size of 11 participants was determined by theoretical saturation — there may be additional ASHA experiences that were not mentioned by the interviewed participants. This points to the need for a more extensive study with more participants. Second, the interviews lasted approximately 30 minutes. To achieve a more nuanced understanding of the ASHAs experiences, the discussion guide might be revised to allow for more questions and a longer conversation. Third, the researchers’ presence during interviews (although unavoidable) may have affected the participants’ responses. Some ASHAs initially thought the research team consisted of members of the Indian government, with the purpose of evaluating their performance. It required some persuasion to convince the ASHAs that we were only there to have a discussion with them and hear their perspective. In a future study, focus group discussions could also be used to facilitate easier conversation.
Conclusion
The four concepts identified by this study are key considerations for the development of the ASHA program. The study highlights the importance of adequate institutional support for the ASHAs and also reaffirms the significance of trusting relationships between the ASHAs and their patients. The added value of the study is that it is based upon the perspectives of the ASHAs themselves and what they perceive as bridges and barriers to fulfilling their roles as grassroots health advocates and community health workers. The ASHAs are remarkable women, and with the right support, have the potential to improve the health of the vulnerable village populations in rural India.
Acknowledgments
Thank you to Farhana Jamal and Pawan Singh Bhadauriya for their consideration of the ASHA. Thanks also go to the ASHAs who gave their valuable time for interviews. The Yale Global Health Field Experience & Seed Funding Awards funded this research.
Sara Locke is a senior in Branford College majoring in History of Science, Medicine & Public Health. Contact her at sara.locke@yale.edu.
__________
References:
1.Team Khushi Baby (2017). 2016 Annual Report. Khushi Baby. Re- trieved from h p://www.khushibaby.org/KhushiBabyAnnualReport_2016.pdf
2. Bajpai, N., Dholakia, R. H. (2011). Improving the performance of Ac- credited Social Health Activists in India. Columbia Global Centers, South Asia, Columbia University, New York (Working Paper No. 1).
3. Fathima, F. N., Raju, M., Varadharajan, K. S., Krishnamurthy, A., Ananthkumar, S. R., & Mony, P. K. (2015). Assessment of “Accredit- ed Social Health Activists”: A national community health volunteer scheme in Karnataka State, India. Journal of Health, Population, and Nutrition, 33(1): 137–145.
4. Indian Ministry of Health and Family Welfare (MoHFW). (2005). NRHM: Mission document. Government of India. Retrieved from: h p:// mohfw.nic.in/NRHM/Documents/NRHM%20Mission%20Document. pdf.
5. Vedm et al. (2011). ASHA–which way forward? Evaluation of ASHA programme in eight states. New Delhi: National Health Systems Resource Centre (NHSRC). 7–10.
6. Gopalan, S. S., Mohanty, S., & Das, A. (2012). Assessing community health workers’ performance motivation: a mixed-methods approach on India’s Accredited Social Health Activists (ASHA) programme. BMJ, 2(5).
7. Singh MK, Singh JV, Ahmad N, Kumari R, Khanna A. (2010). Factors in uencing utilization of ASHA services under NRHM in relation to maternal health in rural Lucknow. Indian Journal of Community Medi- cine, 35: 414-419
8. Rahman SM, Ali NA, Jennings L. (2010). Factors a ecting recruit- ment and retention of community health workers in a newborn care intervention in Bangladesh. Human Resources Health, 8:12.
9. Sco K, Shanker S. (2010). Tying their hands? Institutional obstacles to the success of the ASHA community health worker programme in rural north India. AIDS Care, 22(2): 1606–12.
10. Ritchie, J. (2003). The applications of qualitative methods to social research. In Qualitative research practice – a guide for social science students and researchers (ed. J. Ritchie and J. Lewis), 24-46. Sage Publications, London.
