
BY WEN YI LOW
Imagine you are in a rural clinic in a Zimbabwe village. A child walks in with a fever. Such a fever could be a symptom of any one of a number of life-threatening infectious diseases. There is limited health infrastructure available. There is a lack of storage equipment, access to sophisticated laboratory equipment, and trained workers to conduct or analyze any available diagnostic tests. How can you go about diagnosing and treating this child?
Diagnostics are crucial for the proper identification of both diseases and disease-causing agents, yet tools for diagnosing disease can be expensive, insufficient, or ineffective and can even hinder a patient’s ability to be diagnosed if used improperly. Moreover, despite the key role diagnostics play in healthcare, they tend to receive less attention than novel therapeutics or preventive strategies.1 This issue seems to be improving, with the number of publications on point-of-care tests and diagnostics increasing exponentially from around 100 in 2002 to almost 1000 in 2012.2 Although various research groups have started to pay greater attention to the potential of diagnostics, there are still several challenges to bringing these technologies from the lab to the field.2
Despite the fact that research on novel therapeutics and preventive strategies tends to lead to faster commercialization and greater lucrative rewards than research on diagnostics, the importance of improving diagnostics must not be overlooked. Diagnostics are crucial for identifying the presence and origins of disease. They enable the design of appropriate courses of treatment, measure the effects of interventions, and determine drug resistance or recurrence of existing disease. For therapeutics and preventive strategies to work effectively, there must also be accurate and reliable diagnostics available. Currently, the research and development of new diagnostic tests for illnesses that disproportionately affect low- and middle-income countries are highly dependent on donations from private sources, such as the Bill and Melinda Gates Foundation and pharmaceutical companies.4 This limited funding hinders the development of diagnostic tools that are needed to expedite delivery of treatment and increase chances of survival in resource-limited countries. The insufficient investment can also result in a final cost of USD $2 to 10 million and 5 to 10 years for the development of one new diagnostic test.4 All of this is despite the fact that, at times, the development of a new diagnostic test can be over an order of magnitude more cost-effective than the development of a new drug.4 Hence, there is a need for increased education on and awareness of the importance of diagnostic tests in the global fight against disease.
To be able to quickly, easily, and affordably diagnose diseases, it is necessary to understand the challenges currently facing the developing world that inhibit proper and accurate diagnoses. These challenges include the lack of available resources—human, financial, and energy-related, the lack of proper storage and efficient transportation of samples, the unmet need for trained personnel to conduct and analyze test results, which can lead to variability in the analysis, and the lack of access to appropriate tests. It is essential to develop affordable and efficient tools that can be easily used by healthcare workers in these settings.
While these challenges to development are well-defined, solutions are still required that can meet these constraints. The ASSURED test (Affordable, Sensitive, Specific, User-friendly, Robust, Equipment-free, and Delivered), developed by the World Health Organization to describe the ideal characteristics of a diagnostic test for use in a resource-poor setting, provides a useful guide for designing and developing tools. These criteria are useful for development, but are meant to serve as guidelines, rather than requirements, for effective tests. This is due to the natural variability in the ideal conditions needed for each test, which are dependent on the specific disease and location. For instance, the “equipment-free” criterion is perhaps more applicable to a rural, community setting rather than a local hospital setting where it might be possible to support small-scale equipment. In this case, limiting equipment may serve to constrain the diagnosis rather than improve it.5
Low-cost diagnostic tests that meet the ASSURED criteria can help tackle some of the world’s most pressing health problems and advance global health. Much of the development of these tests is influenced by the research of the Whitesides research group, led by Professor George M. Whitesides of Harvard University, which has developed tools and techniques that are both high-quality and low-cost.6 Like most research on the development of diagnostic tools, Whitesides’ global health research is funded by the Bill and Melinda Gates Foundation. What differentiates Whitesides from other groups is their ability to use this funding to rethink the development of diagnostic tools that are simple and easy to use, by employing a creative and practical approach. As the Director-General of the World Health Organization, Margaret Chan, aptly puts it: “Not all innovation needs rocket science…Given the world’s most pressing health problems, the true genius of innovation these days resides in simplicity.”7 The Whitesides’ focus on simplicity allows them to combine excellent engineering and design with an awareness of the limited resources that are available, to develop diagnostic tools that are reliable, predictable, and consistent.
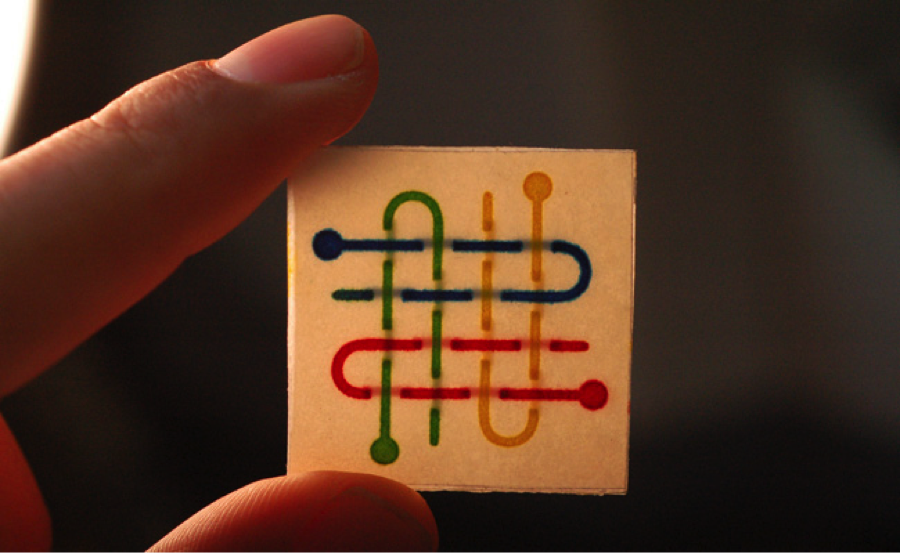
The Whitesides’ simplicity principle has prompted the group to make use of cheap, readily available items in designing high-performance diagnostic systems. One notable technique they have produced is the application of paper-based diagnostics. The inspiration for the design of these diagnostics came from the printing of comic books. By taking advantage of the same inexpensive, large-scale solid wax printing and paper that most comic book manufacturers employ, as well as resources that are already readily available in many places, the complete production of these paper-based diagnostics only requires the designing, printing, and melting of wax paper. Hence, in just three steps, one can print hydrophobic patterns onto the surface of paper, designing channels to direct the flow of liquids. These papers can then be stacked and connected with tape to create 3D microfluidic devices.8 Although the design may be simple, the significance of these paper-based diagnostics should not be underestimated. Prior to this discovery, the construction of precise microchannels for efficient point-of-care diagnostics relied on the use of silicon, a much more expensive material.9 Now, paper-based diagnostics the size of microchips or postage stamps are being created that are cheap and can take advantage of paper’s natural ability to allow the free movement of liquid. Moreover, the paper-based chip can be easily and safely incinerated for disposal, preventing any unnecessary exposure to disease or infection. The Whitesides group has also developed a colorimetric system for these devices, which allows the results to be interpreted by untrained individuals and further improves the cost and simplicity of use in low- and middle-income countries. This invention can help resolve issues with the sorting and classification of fevers of unknown origin. The device contains multiple spots for testing, each of which tests for a marker of a particular disease. These paper-based diagnostic tests have already been employed in India and Vietnam for only USD $0.05 per test, and Dr. Whitesides’ nonprofit engineering company, Diagnostics For All, is continuing to develop and optimize this technology to further improve its potential for use in the field.8 Outside Whitesides, this technology has inspired other research groups to look into researching paper-based diagnostics for various diseases. Engineers at MIT have now developed a paper test that works like a pregnancy test, detecting the presence of specific cancer-associated proteins and revealing within minutes whether a person has cancer.10

The Whitesides group has also worked to develop low-cost storage containers for biological samples. They have pioneered the use of bubble wrap as test tubes to store liquid samples and perform analytical assays. The usage of this packing material as a test tube-like container for medical and environmental samples is highly advantageous in resource-limited areas, because the material is widely available and inexpensive. Additionally, should the bubble wrap break, it will not result in sharp edges that could potentially harm individuals. Bubble wrap can serve as an effective medical storage device because the interior of the bubbles are sterile, allowing the storage of urine, blood samples, or chemicals, without the need for costly autoclaves that require electricity.11 By injecting liquids into these air-filled pockets with syringes and sealing the holes with nail hardener, the bubble wrap can be used to store samples and subsequently, run tests for diseases such as anemia or diabetes. One major obstacle that the Whitesides research group currently faces is that this process for storing samples can be somewhat tedious and requires both syringes and nail hardener, tools that may not be as readily available as bubble wrap. Nevertheless, the Whitesides research group remains optimistic about its material adaptation ideas and believes that it can work to solve this limitation.

In addition to its simple, electricity-free devices, the Whitesides research group has also integrated digital technology into some of the diagnostics it has developed. For example, the group has recently developed the universal Mobile Electrochemical Detector (uMED), a handheld electrochemical detector that can perform chemical analyses and transmit the results to a cloud database from any mobile phone, even low-end models. Data that is collected with this device is transmitted off-site to be analyzed in real time, which allows the comparison of results with those stored in a cloud database and the consultation of a medical expert through text message.12 Moreover, a simple cell phone equipped with a camera can be coupled with other diagnostic tools to make the tools even more simple to use. For instance, a cell phone can be used in combination with a paper diagnostic tool, such that when the colorimetrics have developed after testing, one can take a picture of the device with a cell phone and send it to a central laboratory for analysis. The cost of these diagnostics is then lowered significantly because there is no longer a need for an onsite doctor or trained individual to perform the test analyses.
Development of these low-cost diagnostic tools has tremendous potential to revolutionize the current state of healthcare in the developing world. However, several challenges remain in bringing this technology from the lab to the field. One of the major challenges that research groups face is the lack of funding. While the final diagnostic products that are developed are low-cost, the process of development itself is not cheap.7 Additionally, given the nature of these low-cost diagnostic tools, there is little to no financial incentive for private companies to invest in such research, which makes it even more difficult for research groups to secure funding for development. Academic researchers usually excel in researching these new diagnostic methods and technologies, but they often lack the proper resources, motivation, and experience to execute the trials, regulatory clearance, manufacturing, and quality control necessary to fully develop a product. Thus, there are often research groups who, upon discovering a new technology, seek to sell their product to pharmaceutical companies, hoping that these companies can help bring their inventions into the field. However, when they do agree to invest, pharmaceutical companies tend to have a vested interest in the development of diagnostic tools. For instance, Novartis Pharmaceutical Company and Ciba-Gigy Corporation (the predecessor of Novartis) were at one point accused of having “planned, conspired and colluded to create, develop, and promote the diagnosis of Deficit Disorder to increase the market for its product Ritalin (a drug used to treat ADHD).”13 This pharmaceutical company had a stronger interest in making profits than optimizing the diagnostic tool for use. The success of the Whitesides research group in overcoming this challenge can be largely attributed to its willingness to combine academia, industry, and medicine, all while ensuring its work remains nonprofit. The Whitesides group acknowledged the fact that academic groups excel at basic research and innovation, but lack the key skills needed to bring their product to the field. Thus, Whitesides created a business plan competition at the Harvard Business School, which brought together students at the school and scientists from the group.2 The result, the establishment of the nonprofit organization, Diagnostics for All, Inc. (DFA), ensured that high quality engineering and optimization was maintained while effectively addressing the needs of the developing world.
Diagnostic tools play a key role in advancing the progress of global health. As demonstrated by the Whitesides group, innovative diagnostic tools need not be complex. In fact, the Whitesides’ focus on simplicity and the use of readily available materials has the potential to change how we measure patients’ health conditions in resource-stricken areas and can help overcome the various challenges that prevent low- and middle-income countries from carrying out proper and accurate diagnoses. However, research groups still face several challenges in bringing their products from the lab into the field. Major players in global health should be made aware of the benefits and potential far-reaching impacts of funding research on diagnostic tools, which go beyond the systematic financial gains of the development of such devices.
Wen Yi Low is a visiting international student from the National University of Singapore (NUS) currently in Pierson College and majoring in Chemistry. She can be contacted at wenyi.low@yale.edu.
__________
References:
- Burgess, D. C. H., Wasserman, J., & Dahl, C. A. (2006). Global health diagnostics. Nature, 444, 1-2.
- Kumar, A. A., Hennek, J. W., Smith, B. S., Kumar, S., Beattie, P., Jain, S., Rolland, J. P., Stossel, T.P., Chunda-Liyoka, C.& Whitesides, G. M. (2015). From the Bench to the Field in Low‐Cost Diagnostics: Two Case Studies. Angewandte Chemie International Edition, 54(20), 5836-5853.
- Pitta, D. A., Guesalaga, R., & Marshall, P. (2008). The quest for the fortune at the bottom of the pyramid: potential and challenges. Journal of Consumer Marketing, 25(7), 393-401.
- Mabey, D., Peeling, R. W., Ustianowski, A., & Perkins, M. D. (2004). Tropical infectious diseases: diagnostics for the developing world. Nature Reviews Microbiology, 2(3), 231-240.
- Kettler, H., White, K., & Hawkes, S. (2004). Mapping the landscape of diagnostics for sexually transmitted infections: key findings and recommendations. World Health Organization.
- Whitesides Research Group. (2011). Whitesides Research Group: Research Low-Cost Diagnostics and Tools for Global Health. Retrieved from http://gmwgroup.harvard.edu/research/index.php?page=24.
- Scudellari, M. (2013). A Dime a Dozen. The Scientist. Retrieved from http://www.the-scientist.com/?articles.view/articleNo/33761/title/A-Dime-a-Dozen/.
- Martinez, A. W., Phillips, S. T., Whitesides, G. M., & Carrilho, E. (2009). Diagnostics for the developing world: microfluidic paper-based analytical devices. Analytical chemistry, 82(1), 3-10.
- Chin, C. D., Linder, V., & Sia, S. K. (2012). Commercialization of microfluidic point-of-care diagnostic devices. Lab on a Chip, 12(12), 2118-2134.
- Warren, A. D., Kwong, G. A., Wood, D. K., Lin, K. Y., & Bhatia, S. N. (2014). Point-of-care diagnostics for noncommunicable diseases using synthetic urinary biomarkers and paper microfluidics. Proceedings of the National Academy of Sciences, 111(10), 3671-3676.
- Bwambok, D. K., Christodouleas, D. C., Morin, S. A., Lange, H., Phillips, S. T., & Whitesides, G. M. (2014). Adaptive use of bubble wrap for storing liquid samples and performing analytical assays. Analytical chemistry, 86(15), 7478-7485.
- Nemiroski, A., Christodouleas, D. C., Hennek, J. W., Kumar, A. A., Maxwell, E. J., Fernández-Abedul, M. T., & Whitesides, G. M. (2014). Universal mobile electrochemical detector designed for use in resource-limited applications. Proceedings of the National Academy of Sciences, 111(33), 11984-11989.
- Leavitt, F. (2004). The real drug abusers. Rowman & Littlefield Publishers.
