
BY HANNAH KRYSTAL
Week One
In Bolivia, I stand out as a “gringa.” For most Westerners, this term suggests an insulting inability to blend into the background while on South American soil. But to a native Bolivian, it indicates no more than Western characteristics. Even blond hair can earn a Bolivian born and bred in La Paz the nickname “gringa.” I only discovered this small difference in meaning today during lunch with my host family, and I provide it as an example to demonstrate that I, as a gringa, come to Bolivia with expectations that may often lead to the wrong explanations. As a result, before I describe my experiences in La Paz, I would like to apologize for any mistakes that I make along the way.
I have traveled to Bolivia with the Child Family Health International program. As part of the program, my group splits into teams and spends the morning in el Hospital del Niño, or the Children’s Hospital, of La Paz. Although many believe La Paz to be the capital of Bolivia, Sucre actually holds that title. La Paz is merely home to the Bolivian government (that’s confusing, I know). As a result of its size, people flock to the hospitals of La Paz from various locations in Bolivia, bringing tropical diseases to a place that is far too high above sea level to maintain a mosquito population of its own. Each week, we rotate from unit to unit in the hospital. I have spent my first week in Nephrology, but, for the most part, the patients in that ward fall into the category of General Medicine. The sunny yellow room contains a jumble of diseases, from retinoblastoma to cardiomyopathy to nephritic nephrosis.

The patients range in age from one month to twelve or thirteen years. Many appear months, or even years, younger than the ages posted alongside their names and diagnoses on the signs taped to the feet of their beds. Today, I mistook a seven-year-old for a four-year-old. The girl’s scoliosis had shortened her spine, and other developmental delays left her wordlessly terrified as the nurses wheeled her away for yet another surgery. A second girl in the ward could easily pass as younger than ten months old, yet she will turn three in December. She recently learned to roll onto her side, but she cannot speak or even crawl, let alone walk. Many of the children’s disabilities result from a critical lack of mental and physical stimulation. The ward cannot afford soap or toilet paper, let alone books or crayons and paper. My partner and I brought some coloring books to the older children the other day, and they hoarded each design carefully, knowing that it would not easily be replaced, despite the cheapness of the supplies. Most mothers, and sometimes a father or two, sit beside their babies on padded brown chairs covered in cracking plastic, but most parents cannot afford to do more for their children’s entertainment than shake a rattle, talk, or play some music on their phones. The almost three-year-old was the only exception; her birth mother abandoned her in the hospital when she was only five months old. But an incredible woman has stepped in, and is currently in the process of adopting the child. I wish her the best of luck.
Because the only curtains in the ward barely cover the windows, there is no privacy. The open atmosphere allows the children, and the mothers, to grow close. Often, the mothers will care for each other’s children, or sit together and chat as they watch their children play. The children not only play together, but also look out for each other. One eight-year-old boy watches over the almost three-year-old like an intensely protective older brother. This system, however, has its disadvantages. After one child’s mother fed him yogurt for lunch, four other children sat beside him at the small, rickety table in the middle of the room as he quietly vomited into the bowl his mother brought for him, because food is scarce. The Bolivian healthcare system allegedly pays for all treatments for children under five years of age, but it cannot afford the basic amenities. Breakfast consists of a roll or crackers dipped in a bowl of bread dissolved in milk, and a large chunk of papaya can serve as lunch. Baths, if they are given, consist of water with no form of surfactant.
Because my ward is basically General Medicine, it has been relatively quiet. The almost three year old, who has a tracheal tube, cries silently as the nurses clear her tube of the phlegm that causes her breathing to hitch painfully. To remove the phlegm, the nurses stick a small plastic tube attached to a vacuum into the one taped to the girl’s throat, essentially choking her for minutes at a time. The cleaning ritual occurs several times daily. The babies in the ward often cry as well, although they wail so weakly one could almost walk by without noticing. Many of the children suffer from cavities, but these remain untreated. One boy, for example, basically has one front tooth because the two in his mouth are so rotted that only half of each remains. The decay has also spread to the one adult tooth peeking out from his gum on the left side, suggesting that not much hope remains for his dental hygiene even after his baby teeth fall out. Because the ward does not supply toothpaste and the tap water would probably cause as many diseases as it would prevent, poor dental hygiene in the ward is an unsurprising norm.
Today, my fourth day in the ward, a man and a woman suddenly walked in and began singing to the children. I am not sure whether they were paid singers or volunteers, or about the regularity of their performances, but their presence reminded me of all of the visits that children in the United States of America receive during the holidays. I hope that the singers come often, and, since today was not a holiday, perhaps they do. The nurses spend the most time with the children and seem deeply invested in their well being, although I have yet to see one use a pair of gloves. I have heard from a group of CFHI students on the surgery rotation that the surgeons use gloves, but even the anesthesiologist who prepares the patient for surgery does not. To sum up my first week, the best of intentions attempt to make up for the incredibly pervasive level of poverty, creating a scene of heart wrenching failures mixed with consistent examples of human kindness.
Week Two
Warning: graphic content
Originally, I intended to write this post about rounds, about the doctors who push around a desk containing one or more typewriters, who speak in whispers because they stand within hearing range of almost every patient in the room.
But then, Infectology received a new patient. She was a spillover from an unspecified department, although Psychology or Gynecology seemed like they would have been the best choices for her. Two days before, the fourteen-year-old girl had entered a cab with a boy she had just met a few days before. The two of them met up with another male friend, and the boys plied her with rum and coke. She pleaded to go to school, but they ignored her. She blacked out, and woke up the next morning with defensive wounds on her palms, arms, and face. She had been raped.
I am sure that this incident could occur anywhere in the world. To me, though, one of the tragic aspects of her case was the inability of the hospital to properly take care of her once she had escaped her rapists. The doctors knew exactly which medications they needed to prevent the various STDs that the rapists may have given her, but they lacked proper access. They had no HPV vaccine, so if the rapists had that disease, she would get it, too. And, because Bolivians consider abortion to be a sin, the girl faced more than HepA or HPV. If she became pregnant, she most likely will keep the baby.
Similar situations occur throughout the hospital daily, because the public hospitals do not have access to vaccines that ward off HepA, measles, mumps, or chicken pox, to name a few. A boy in the ward, whose jaundice is clearly visible, was sent home after a nasty case of HepA. I’m not sure if he was cured, because he still has jaundice and they talked about the high mortality rate of cases like his. Instead, I fear that he went home to die.
As Americans choose to ignore their miraculous access to the latest vaccines and desperately try to curtail their access to abortions, it is horrible to watch the desperation of Bolivians as they dream, or fail to dream, of those same tossed-aside lifesavers. Vaccination exemptions look even more ridiculous here than they do at home, similar to the attempts to curtail abortion clinics that make me burn with frustration. Just as some Bolivians still believe that diarrhea should be treated with dehydration to stem the flow of fluid, American education about vaccines and sex has clearly failed the public. I wish that Americans would learn to appreciate, instead of fear, vaccines, because Bolivia represents a tale of caution about herd immunity and its lack. Both countries also need to learn to appreciate the burden of an unexpected child.
Week Three
It seems like most surgeries here correct problems much more easily solved by preventative care. As I watched the surgeon saw aggressively through the thigh of a two year old girl, he told me, with what seemed to be pride, that they would never attempt this type of surgery where I come from because the pediatric care is better. They would notice that the girl’s femur was misaligned, and correct the issue before it became necessary to cut through her thigh muscle, capsule, and tendon in order to properly place her bone in its socket. In fact, Americans would never injure their children in this manner because they use different equipment to carry their babies around. This injury is extremely common in Bolivia because the women wrap their babies in blankets until they are locked in place like mummies, and then tie them to their backs using large, colorful sheets. The mummification process leads to hip dysplasia such as that suffered by this patient, because the babies’ legs are not allowed to move or develop normally. The procedure required to fix the dysplasia would leave the toddler in a cast attached to a wooden pole with her legs spread apart in midair for six months.
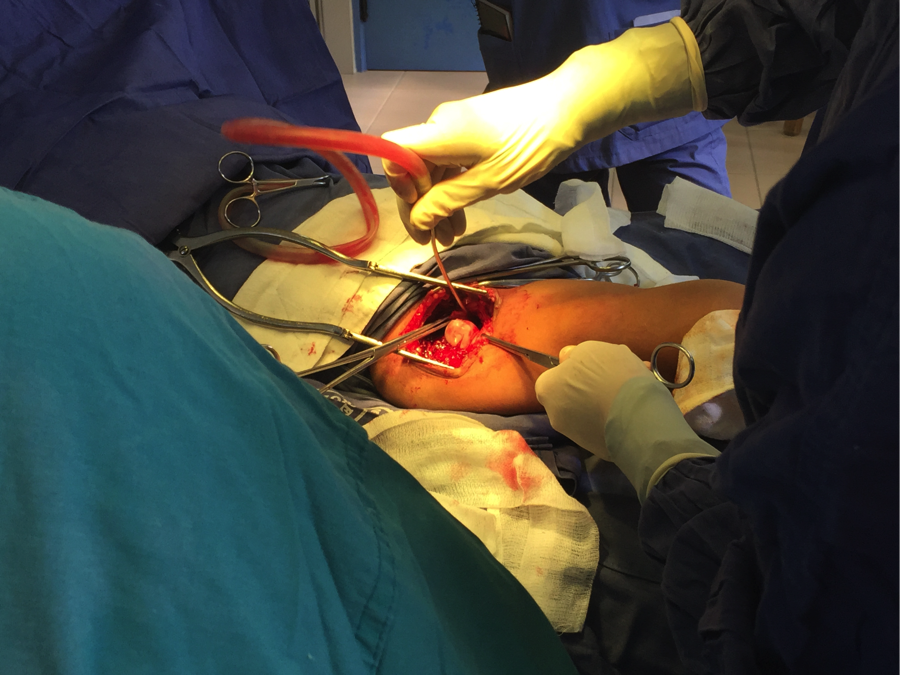
During the procedure, the surgeon moved indelicately, to say the least. At one point, he cut into her muscle so quickly that a vein spurted out onto the floor behind him, and onto my protective bootie beyond that. There were perhaps two centimeters between the end of my bootie, my magically unstained shoe, and my stained pants. I was shocked, but the doctor hardly noticed as he fingered broken muscle and told me that the blood pooling out of the wound was “nothing,” not nearly enough to warrant a transfusion.
That doctor was not the one I regularly shadow, because my shadow-ee moved much more cautiously. But, without any ultrasound, x-Ray, or scanning technology, even the gentler doctor had been forced to pull the entire liver out of a five year old girl’s abdomen in order to search for its five cysts, ranging in size from a hacky sack to an iPhone 6 plus, the day before. In the process, her appendix fell out of one of the slits used to find, destroy, and remove the cysts, so the doctor removed it as well. He told me that the risk of infection from exposure to the air was too high to just push it back inside and hope for the best.
Last night, I talked with my host brother, and we discussed the state of health care in our respective countries. He told me that the callous behavior of the doctor was all the more tragic because the spirit of Latin America is much warmer than that of the States. Look at the Pope for an example, he said. The Pope is a man of the people. The doctors here have to work with many fewer tools and therefore have a much more hands-on, bloody experience. There are no ultrasounds to check for cysts, and no microscopes to ensure that the margins of the tumor are clear of cancerous cells. Very few people beyond the surgeons, including the anesthesiologists, use gloves. With that much painful patient contact, it must be difficult to face patient care each day without becoming jaded.
Week Four

On Friday morning, I discovered the ambulatory care room in the Oncology ward. This was where all the cries I had heard during the week had originated, and where all of the action happened. I watched one paraplegic boy receive his chemotherapy in an extremely painful manner. The mother had his chemotherapy bags in her purse, and she pulled them out for the nurses. First, the nurses placed the needle in his arm, and then connected the needle to the air-filled tube that was supposed to bring the medicine to the patient. But one tube, two tubes, and then a second bag of chemotherapy later, the boy had not yet received his medicine. Instead of medicine dripping into his arm, blood was leaking into the tube. The nurses decided to inject the medicine with a syringe instead of waiting for the IV drip any longer, so they sloppily poured the medicine into a syringe. They injected the contents of the first bag, and then halfway through the second bag, a nurse dropped a syringe full of medicine onto the floor. They injected what was left of the dirty syringe’s contents into the boy’s arm and then injected a third bag’s supply, as well. As usual, no air bubbles were removed before injecting the treatment. The boy never cried out in pain, suggesting that he was used to the treatment because he had received no pain medication before or during this process. Later, the doctor took one look at a bag of chemotherapy and declared it perfectly normal, suggesting that someone, somewhere along the line, had screwed up. I’m still not sure exactly what went wrong when the nurses tried to deliver the medicine the first time, but I do believe that time sensitive chemotherapy should not be delivered through a syringe, and that families should not be responsible for holding onto their children’s syringes and chemotherapy. I don’t know why they send the medications home, but it seems like a misadventure waiting to happen.
Week Five
Today was my last day in el Hospital del Niño, so I wanted to end my stories about the hospital on a positive note. I have spent this past week in Pneumology, also known as Pulmonology. Like Nephrology, it has open wards. This past week, two mothers in the ward have shown me the Latin American warmth of which my host brother was so proud. One of the women, another “soltera,” (“unmarried”) mother, is sixteen years old. The mother of the baby in the next bed, who is slightly older than her companion, keeps the girl company as she sits beside her baby each day. Despite waiting for months in the hospital, they still have been extremely kind to the bumbling intern whom they have only known for a week. Both women, when they found out that I was leaving, asked me for hugs and photos. I only hope that they friend me on Facebook, so that I can share their kids’ cuteness on this blog.
Week Six
This was my last week in Bolivia, so instead of going back to el Hospital del Niño, I went to a primary healthcare clinic in El Alto. El Alto, as its name suggests, encircles the valley of La Paz. Because the real estate is higher, it is also cheaper. El Alto, therefore, is home to La Paz’s poorest citizens. I saw some fascinating cases, from a baby girl with six toes on her right foot to a baby boy whose mother, despite having successfully raised his adolescent brother, failed to properly burp him. When the doctor tapped his stomach, the taut skin reverberated like a drum.
The doctor works every day with young babies and expectant mothers. These mothers range in age from fifteen to thirty-eight (to my knowledge; there are most likely mothers both older and younger who have heard their babies’ hearts beat on the bed in the corner). But the doctor, who constantly advocates for family planning and contraceptive use, saying, “go get some condoms” or “have you started family planning yet? You already have four little ones!” is herself a single mother. She became pregnant while still in school, and, thanks to her mother, was able to stay in school while raising her child. She has since remained single because of the machismo culture in Bolivia. She says that men are taught that it is acceptable to beat women, and women that they must stay silent about their abuse. Even the doctor’s daughter experienced abuse at the hands of her husband, a lawyer. But, yet again, the doctor and her family rose above their difficult circumstances. The daughter divorced her abusive husband, and the doctor, like her mother before her, now devotes herself to helping her child raise her own baby. This demonstration of self-empowerment is so inspiring to me because few women here have successfully risen above the expectations that a woman must be married and that a woman should not fight back against domestic abuse. Often, the cause of this failure challenge the typical Bolivian female role is the unexpected product of rape, because abortion is very strongly frowned upon in Catholic Bolivia. (Before the Pope came to visit La Paz on July 8th, for four hours total, La Paz spent more than a month preparing for his arrival with news stories about “El Papa en Bolivia.” News about the Pope always ended with a special theme song.)
Stories like these, and not merely unlikely scenarios in which a bartender asks “how are you doing tonight?” as we saw during bystander training this past year, seem like the fodder for better sexual assault training on college campuses. Women would be able to look at the consequences of not speaking out about sexual assault, and learn to appreciate their on-campus resources more strongly. Men could take a second look at the machismo culture that exists in the States, as well as Bolivia. It seems cruel to use these stories as no more than look-how-far-we’ve-come anecdotes, but living in Bolivia has truly made me appreciate the resources I have in America, and I wish that everyone could have the same experience with the fight to end sexual assault. Anti-violence signs paper the streets, but I witnessed a domestic abuse case on one of those streets during my first week in Bolivia. Three men were surrounding a woman and hit her repeatedly, but, even though a man in a nearby car was shouting at them, she cried quietly instead of crying out for help. The doctor was able to bring her daughter out of a situation that might have been very similar, but most women say nothing. For me to say nothing about the hardships I have witnessed here would be to relegate the women’s stories to the same dark fate as their unhealthy relationships (usually marriage, but lately couples who chose not to be married are made up of a man and a “concubine”). I want to tell these stories so that no more of them will wreak havoc on the lives of women worldwide.
