
BY ALY MOORE.
Photography and Graphics by Aly Moore.

In 2005, only 32,875 people were hospitalized or given outpatient consultations in Ghana, representing a 98% treatment gap. Although mental, neurological, and substance use disorders combine for up to 13% of the global burden of disease, only an estimated 3.6% of Ghana’s current health budget is allocated for mental health. John Mahama, the current president of Ghana, has spoken at length about raising awareness to change the current attitude of “mental health [as] an afterthought.” Mahama started by making the Ministry of Health and the Ghana Health Service launch a national campaign to raise awareness about mental health and reduce stigma associated with mental health patients.
In August 2011, President Mahama assured citizens that mental health would be adequately addressed in the government’s plans to upgrade all national, regional and district health facilities. Mahama met with a group of Ghanaians who had attended the Yale Global Health Leadership Institute (GHLI) conference, where they focused on ways to address the rising mental health problems in their country.
The journey through the Ghanaian mental health system started for me when I met Patrick Geoghegan OBE, then-CEO of the South Essex Partnership and Trust (SEPT). His passion for global health inspired my journey to England the following summer to work for SEPT.
In England, I worked on Patrick’s ongoing project with the SEPT Global Health Charity in Ghana, conducting intensive research on the status of the Mental Health Bill in Ghana. I was given the opportunity to interview the key players in development and improvement of psychiatric hospitals in Ghana and charged with producing a report with the potential to truly impact policy. The report is structured in two sections: The first describes SEPT’s achievements in Ghana while the second critically analyzes unfinished policy work.
SEPT Global Health Charity was founded in October 2010 to raise funds to send a container of medical supplies and equipment to the Pantang Hospital in Accra, Ghana. It has since sent eight 20-foot containers and raised a staggering £25,000 to support the improvement of the mental health facilities at Pantang Hospital. The funds raised were largely used to cover the cost of shipping the containers to the Ghanaian facilities, while the contents of the containers were donated by SEPT, including necessary living-space improvements such as furniture and medical supplies such as syringes, drug trolleys, and cannulas.
While these items are often taken for granted in the UK, in the Pantang Hospital, they were treasures. According to one of the Pantang physicians, Dr. Anna Puklo-Dzadey, ,“The contents of the containers will help provide some of the most basic things that those in the developed world would take for granted and will go a long way to improving patient care and comfort. I’m extremely grateful to Patrick for arranging the shipment to us and thank the staff of SEPT for doing their bit to help.” Beyond physical supplies, the containers brought hope, motivation and joy to the staff and patients at the Pantang Hospital.
SEPT also raised enough funds to purchase 20 beds, at a cost of £200.00 for each bed complete with bedding, to furnish a new assessment ward, which Patrick proudly opened in December of 2010.
The Mental Health Bill
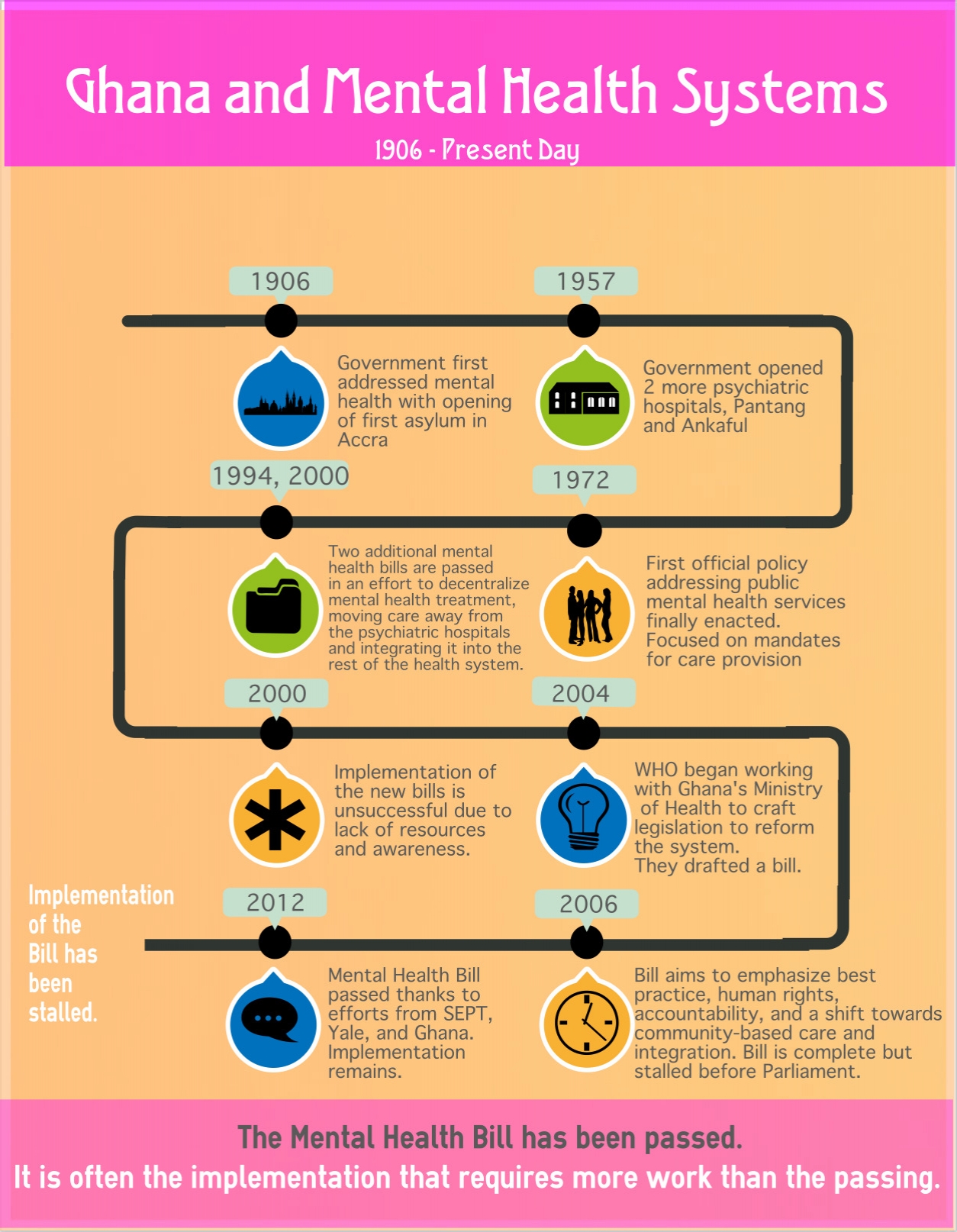
As relationships with the various members of Pantang Hospital, Accra, Ghana and Yale grew, Patrick became involved in the collaborative effort to help pass and implement new mental health policy in Ghana. In 2004, the WHO began working with Ghana’s Ministry of Health to craft legislative reform for the country’s mental health system, based on WHO guidelines. Together they drafted a bill that, while providing few specifics about patient care and facility staffing, presented a new vision for the mental health system. The bill emphasized best practices for treatment, respect for human rights, accountability, and a shift from institutional care toward community-based treatment and integration of mental health into general medical practice. While completed in 2006, the bill tragically stalled before Parliament. However, with the added weight of international interest in recent years, the Ghana Mental Health Bill was passed on March 3, 2012. If the bill is properly implemented, the legislation has the potential to serve as a model for other countries in West Africa, or, more broadly, other low-income countries working to strengthen mental health services.
Although passage of the 2012 Ghana Mental Health Bill was a major milestone, it did not expand and enhance the workforce enough to implement the provisions set forth within and improve upon current mental health services. The bill also relies on a substantial amount of additional funding and administrative action, which has not been forthcoming.
An ongoing Supreme Court case examining the legitimacy of President John Mahama’s administration continues to monopolize national attention. The trials are broadcast live on television, and the population of Ghana watches eagerly, since the country’s future hinges in no small part on the ruling. Perri Kasen, 2013 GHLI Fellow, comments, “Though entirely fascinating… the Supreme Court case has created huge roadblocks in implementing the Mental Health Bill, as many action items require Presidential approval.”
The current hold-ups with the bill concern more than just the president. Ghana is faced with a significant capacity issue as well as a training issue – do the people that are required to implement the new provisions have the requisite political expertise to complement their clinical training? Ghana will need a knowledgeable individual to single-mindedly pursue the next steps for mental health, pushing the bill forward and providing a tangible plan for the future. As of yet, no one has stepped forward.
While the majority of the bill has yet to be enacted, the successes of smaller scale projects give reason to celebrate. Collaboration with Yale and SEPT has encouraged the exchange of models and ideas and Patrick is currently working to continue this interplay through an academic exchange between the physicians within the different countries. Hopefully, the doctors of Ghana will take back models of care, such as the structure of Assessment Wards, which will improve patient conditions and lead to lessened stigma. Reciprocally, doctors from the U.S. and England could learn much on the ground in Ghana. Ghanaian physicians are very proud of their ability to work within the suboptimal conditions they are given; they have avoided any major Cholera outbreaks, for example, in a facility without running water.
My experience with SEPT shows the need to focus on implementation as the necessary follow up for policy change. Passing the bill was the easy part; we must recommit to improving mental health in Ghana as we move from policy to reality.
[1] Mental Health Bill, (21 July, 2010).
[1] Jack, Helen. “There is no motivation here: Exploring how to expand mental health care services in Ghana by addressing the needs of the workforce.” Assets, Poverty, and Inequality II Dissertation, December 9, 2011.
